


Has The Primary Cause Of Cancer Been Hidden?
Just Like Diabetes And Heart Disease

In my previous post Diabetes Has A Hidden Cause I exposed the deliberately hidden reasons for the explosion of diabetes illness and death in many millions of people on the Earth.
Below is a link to that post:
Diabetes Has A Hidden Cause
Unfortunately for the many millions who have been injured or died, as well as their grieving relatives, the history of the explosive expansion of cancer throughout the world, has similar roots to the hidden diabetes story.
On October 8, 1883, a son was born to Emil Warburg, a prominent Jewish physicist in Freiburg, Germany. When he was thirteen, the family moved to Berlin, where visitors to his parents’ home included some of the giants of the natural sciences—chemist Emil Fischer, physical chemist Walter Nernst, physiologist Theodor Wilhelm Engelmann.
No one was surprised when young Otto, growing up in such an atmosphere, enrolled in the University of Freiburg to study chemistry. But by the time he received his Ph.D. in 1906, a growing disease epidemic had caught the attention of this ambitious young man. His was the first generation seriously to be affected by it.
That disease was cancer.
Cancer rates all over Europe had doubled since he was born, and he determined to devote his life to finding the reason and, hopefully, a cure. With this in mind he returned to school, receiving his M.D. from the University of Heidelberg in 1911.

Otto Heinrich Warburg, M.D., Ph.D. (1883-1970)
What fundamental changes, he wondered, take place in the tissue when a normal cell becomes cancerous? “Does the metabolism of tumors,” he asked, “growing in a disorganized manner, differ from the metabolism of orderly cells growing at the same rate?” Impressed that both tumors and early embryos consist of undifferentiated cells that multiply rapidly, Otto Warburg began his life’s work by studying fertilized eggs. Perhaps, he speculated, cancer cells are just normal cells that have reverted to an embryonic pattern of growth. He chose the sea urchin egg to study because its embryo is large and grows particularly fast. His first major work, published while he was still in medical school, showed that on fertilization the rate of oxygen consumption of an egg rises sixfold.
But in 1908, he could pursue his ambition no further because the chemical reactions within cells that involve oxygen were completely unknown. Spectrophotometry—the identification of chemicals from the frequencies of light they absorb—was new, and had not yet been applied to living systems.
Existing techniques for culturing cells and measuring gas exchange were primitive. Warburg realized that before any real progress could be made in elucidating the metabolism of cancer, fundamental research on the metabolism of normal cells would have to be done. Cancer research would have to wait.
During the coming years, Warburg, using techniques that he developed, proved that respiration in a cell took place in tiny structures that he called “grana” and that we now call mitochondria. He experimented with the effects of alcohols, cyanide, and other chemicals on respiration and concluded that the enzymes in the “grana” must contain a heavy metal that he suspected, and later proved, was iron. He conducted landmark experiments using spectrophotometry that proved that the portion of the enzyme that reacts with oxygen in a cell is identical with the portion of hemoglobin that binds oxygen in the blood. That chemical, called heme, is a porphyrin bonded to iron, and the enzyme containing it, which exists in every cell and makes breathing possible, is known today as cytochrome oxidase. For this work Warburg was awarded the Nobel Prize in Physiology or Medicine in 1931.
Mitochondria
Meanwhile, in 1923, Warburg resumed his research on cancer, picking up where he had left off fifteen years earlier. “The starting point,” he wrote, “has been the fact that the respiration of sea urchin eggs increases six-fold at the moment of fertilization,” i.e. at the moment that it changes from a state of rest to a state of growth. He expected to find a similar increase of respiration in cancer cells. But to his amazement, he found just the opposite. The rat tumor he was working with used considerably less oxygen than normal tissues from healthy rats.
“This result seemed so startling,” he wrote, “that the assumption seemed justified that the tumor lacked suitable material for combustion.” So Warburg added various nutrients to the culture medium, still expecting to see a dramatic rise in oxygen use. Instead, when he added glucose, the tumor’s respiration ceased completely! And in trying to discover why this happened, he found that tremendous amounts of lactic acid were accumulating in the culture medium. The tumor, in fact, was producing fully twelve percent of its weight in lactic acid per hour. Per unit time, it was producing 124 times as much lactic acid as blood, 200 times as much as a frog’s muscle at rest, and eight times as much as a frog’s muscle working to the limit of its capacity. The tumor was consuming the glucose, all right, but it was not making use of oxygen to do it.
In additional experiments on other types of cancers in animals and humans, Warburg found that this was generally true of all cancer cells, and of no normal cells. This singular fact impressed Warburg as of utmost importance and the key to the causation of this disease.
The extraction of energy from glucose without using oxygen, a type of metabolism called anaerobic glycolysis—also called fermentation—is a highly inefficient process that takes place to a small extent in most living cells but only becomes important when not enough oxygen is available.
For example, runners, during a sprint, push their muscles to use energy faster than their lungs can deliver oxygen to them. Their muscles temporarily produce energy anaerobically (without oxygen), incurring an oxygen debt that is repaid when they end their sprint and stop to gulp air. Although capable of supplying energy rapidly in an emergency, anaerobic glycolysis produces much less energy for the same amount of glucose, and deposits lactic acid in the tissues that has to be disposed of.
Some primitive forms of life today—many bacteria and yeasts, for example—rely on anaerobic glycolysis.
What Warburg discovered in 1923 is that cancer cells differ from normal cells in all higher organisms in this fundamental respect: they maintain high rates of anaerobic glycolysis and produce large amounts of lactic acid even in the presence of oxygen. This discovery, called the Warburg effect, is the basis for the diagnosis and staging of cancer today, using positron emission tomography, or PET scanning. Because anaerobic glycolysis is inefficient and consumes glucose at a tremendous rate, PET scans can easily find tumors in the body by the more rapid uptake of radioactive glucose. And the more malignant the tumor, the more rapidly it takes up glucose.
Warburg reasonably believed he had discovered the cause of cancer. Evidently, in cancer, the respiratory mechanism has been damaged and has lost control over the metabolism of the cell.
Unrestrained glycolysis—and unrestrained growth—are the result. In the absence of normal metabolic control the cell reverts to a more primitive state. All complex organisms, proposed Warburg, must have oxygen in order to maintain their highly differentiated forms. Without oxygen, they will revert to a more undifferentiated, simple form of growth.
“The causative factor in the origin of tumors,” proposed Warburg, “is nothing other than oxygen deficiency.” When cells are deprived of oxygen only temporarily, glycolysis takes over during the emergency, but ceases again when oxygen is once more available. But when cells are repeatedly or chronically deprived of oxygen, he said, respiratory control is eventually damaged and glycolysis becomes independent. “If respiration of a growing cell is disturbed,” wrote Warburg in 1930, “as a rule the cell dies. If it does not die, a tumor cell results.”
Warburg’s theory was controversial from the beginning. Hundreds of different kinds of cancers were known in the 1920s, triggered by thousands of kinds of chemical and physical agents. Many scientists were reluctant to believe in a common cause that was so simple. Warburg answered them with a simple explanation: each of those thousands of chemicals and agents, in its own way, starves cells of oxygen. Arsenic, he explained by way of example, is a respiratory poison that causes cancer.
Urethane is a narcotic that inhibits respiration and causes cancer. When you implant a foreign object under the skin, it causes cancer because it blocks blood circulation, starving neighboring tissues of oxygen.
Although they didn’t necessarily accept Warburg’s theory of causation, other researchers lost little time confirming the Warburg effect. Tumors did, universally, have the ability to grow without oxygen. By 1942, Dean Burk at the National Cancer Institute was able to report that this was true of over 95 percent of the cancerous tissues he had examined.
Then, in the early 1950s, Harry Goldblatt and Gladys Cameron, at the Institute for Medical Research at Cedars of Lebanon Hospital in Los Angeles, reported to a skeptical public that they had succeeded in transforming normal cells—cultured fibroblasts from the heart of a five-day-old rat—into cancer cells merely by repeatedly depriving them of oxygen.
In 1967, Burk’s team proved that the more malignant a tumor is, the higher its rate of glycolysis, the more glucose it consumes, and the more lactic acid it produces. “The extreme forms of rapidly growing ascites cancer cells,” Burk reported, “can produce lactic acid from glucose anaerobically at a sustained rate probably faster than any other living mammalian tissue—up to half the tissue dry weight per hour. Even a hummingbird, whose wings may beat up to at least one hundred times a second, consumes at best only half its dry weight of glucose equivalent per day.”
Because he insisted that the origin of cancer was known, Warburg thought that “one could prevent about 80 percent of all cancers if one could keep out the known carcinogens.” He therefore advocated, in 1954, for restrictions on cigarette smoking, pesticides, food additives, and air pollution by car exhaust. His incorporation of these attitudes into his personal life earned him a reputation as an eccentric. Long before environmentalism was popular, Warburg had a one-acre organic garden, obtained milk from an organically maintained herd, and purchased French butter because in France the use of herbicides and pesticides was more strictly controlled than in Germany.
Otto Warburg passed away in 1970 at the age of 83—the same year the first oncogene was discovered. An oncogene is an abnormal gene, thought to be caused by mutation, that is associated with the development of cancer. The discovery of oncogenes and tumor suppressor genes promoted a widespread belief that cancer was caused by genetic mutations and not by altered metabolism.
Warburg’s hypothesis, controversial from the start, was largely abandoned for three decades.
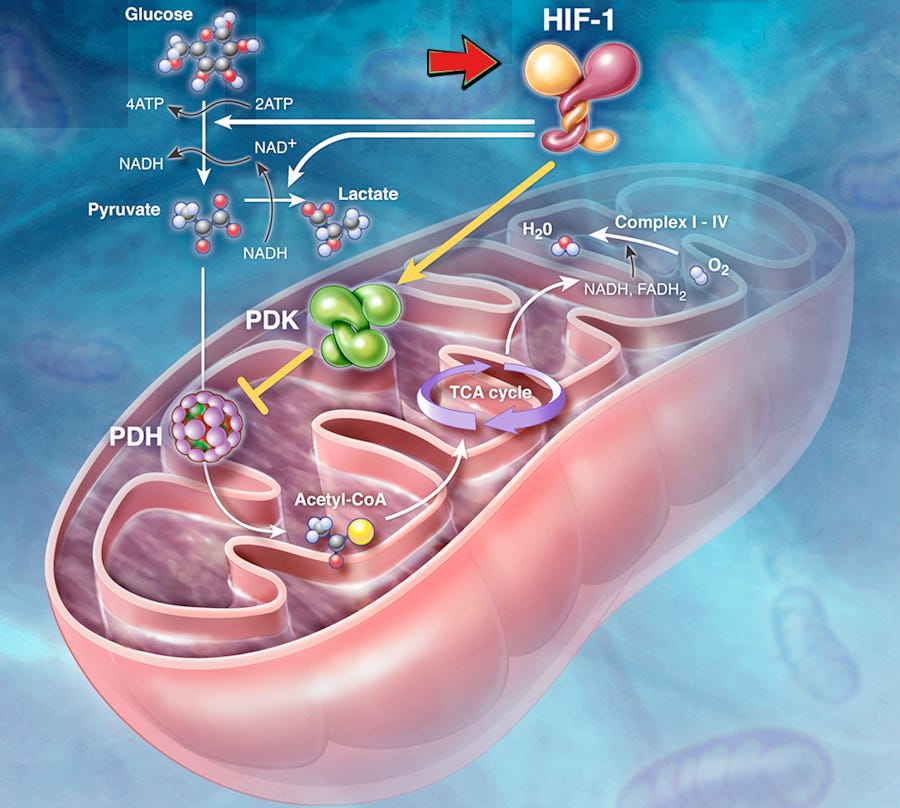
But the widespread use of PET scanning for diagnosing and staging human cancers has catapulted the Warburg effect back onto the main stage of cancer research. No one can now deny that cancers live in anaerobic environments, and that they rely on anaerobic metabolism in order to grow. Even molecular biologists, who once focused exclusively on the oncogene theory, are discovering, after all, that there is a connection between lack of oxygen and cancer. A protein has been discovered that exists in all cells—hypoxia-inducible factor (HIF)—that is activated under conditions of low oxygen, and that in turn activates many of the genes necessary for cancer growth.
HIF activity has been found to be elevated in colon, breast, gastric, lung, skin, esophageal, uterine, ovarian, pancreatic, prostate, renal, stomach, and brain cancers.
Cellular changes that indicate damaged respiration—including reductions in the number and size of mitochondria, abnormal structure of mitochondria, lessened activity of Krebs cycle enzymes, lessened activity of the electron transport chain, and mutations of mitochondrial genes—are being routinely found in most types of cancer.
Experimentally inhibiting the respiration of cancer cells, or simply depriving them of oxygen, has been shown to alter the expression of hundreds of genes that are involved in malignant transformation and cancer growth. Damaging respiration makes cancer cells more invasive; restoring normal respiration makes them less invasive.
A consensus is forming among cancer researchers: tumors can only develop if cellular respiration is diminished.
In 2009, a book dedicated to Otto Warburg was published titled “Cellular Respiration and Carcinogenesis.” Addressing all aspects of this question, it contains contributions from leading cancer researchers from the United States, Germany, France, Italy, Brazil, Japan, and Poland. In the foreword, Gregg Semenza wrote: “Warburg invented a device, now known as the Warburg manometer, with which he demonstrated that tumor cells consume less oxygen (and produce more lactate) than do normal cells under the same ambient oxygen concentrations. A century later, the struggle to understand how and why metastatic cancer cells manifest the Warburg effect is still ongoing.
The question being asked today by cancer researchers is no longer, “Is the Warburg effect real?” but “Is hypoxia a cause, or an effect, of cancer?” But, as increasingly many scientists are admitting, it really doesn’t matter, and may be only a question of semantics. Since cancer cells thrive in the absence of oxygen, oxygen deprivation gives incipient cancer cells a survival advantage. And any environmental factor that damages respiration therefore—whether Warburg was right and it directly causes malignant transformation or whether the skeptics are right and it merely provides an environment in which cancer has an advantage over normal cells—will necessarily increase the cancer rate.
Electricity is such an environmental factor.
Under the influence of electromagnetic fields, respiratory enzyme activity is slower. After a meal, the cells cannot oxidize the breakdown products of the proteins, fats, and sugars that we eat as quickly as they are being supplied by the blood. Supply outstrips demand. Recent research has shown exactly how this happens.
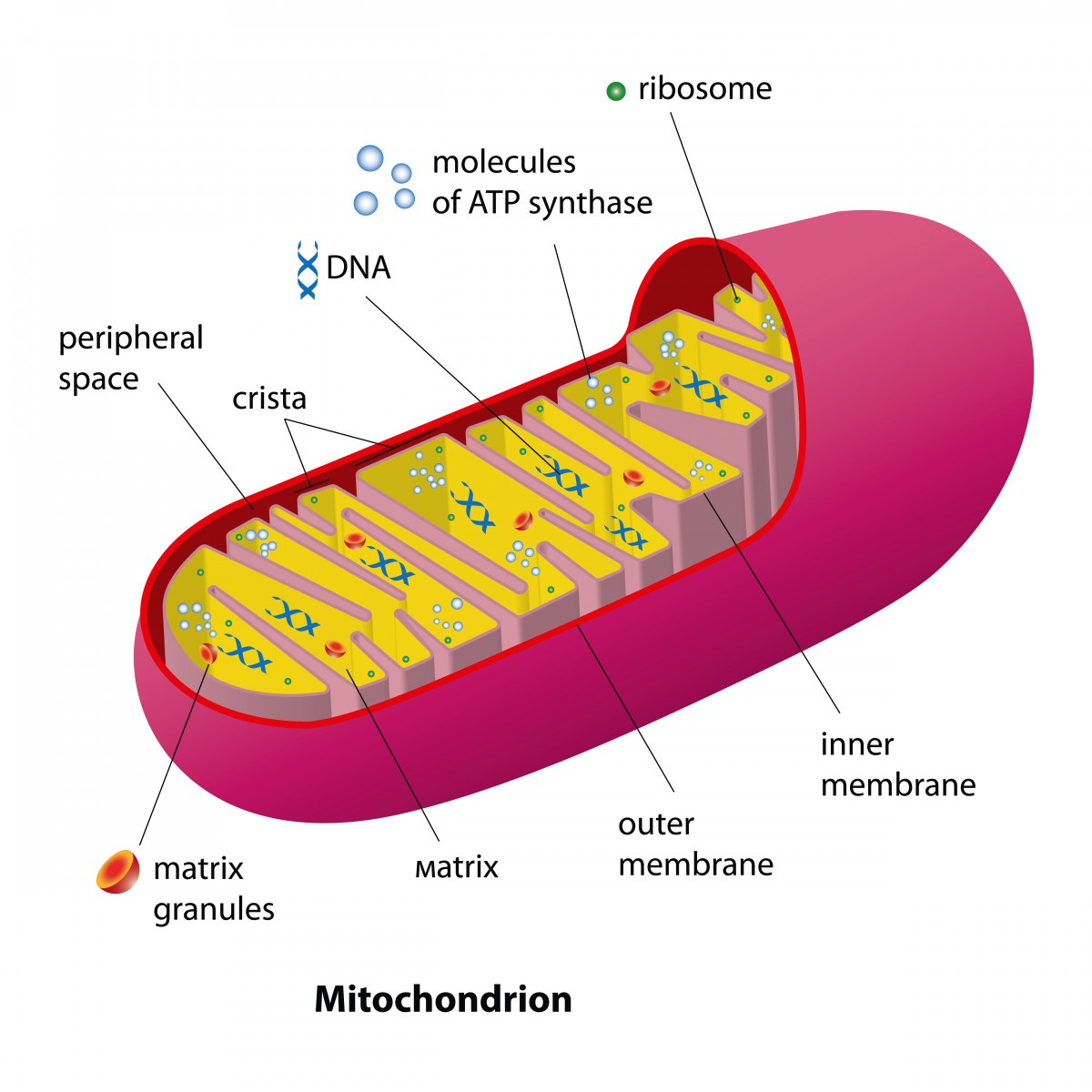
Inside the mitochondria, amino acids, fatty acids, and glucose are all further transformed into even simpler chemicals that feed into a common cellular laboratory called the Krebs cycle, which breaks them down the rest of the way so that they can combine with the oxygen we breathe to produce carbon dioxide, water, and energy. The last component in this process of combustion, the electron transport chain, receives electrons from the Krebs cycle and delivers them, one at a time, to molecules of oxygen. If the speed of those electrons is modified by external electromagnetic fields, or if the functioning of any of the elements of the electron transport chain is otherwise altered, the final combustion of our food is impaired. Proteins, fats, and carbohydrates begin to compete with each other and back up into the bloodstream. Fats are deposited in arteries. Glucose is excreted in urine. The brain, heart, muscles, and organs become oxygen-deprived. Life slows down and breaks down.
If the same cause—a slowing of metabolism by the electromagnetic fields around us—produces both diabetes and cancer, then one might expect diabetics to have a high rate of cancer, and vice versa. And it is so.
The first person to confirm a connection between the two diseases was South African physician George Darell Maynard in 1910. Unlike almost all other diseases, rates of both cancer and diabetes were steadily rising. Thinking that they might have a common cause, he analyzed mortality statistics from the 15 death registration states in the 1900 Census of the United States. And he found, after correcting for population and age, that the two diseases were strongly related. States that had higher incidences of one also had higher incidences of the other. He proposed that electricity might be that common cause:
“Only one cause, it seems to me, will fit the facts as we know them, viz.: the pressure of modern civilization and the strain of modern competition, or some factor closely associated with these. Radio-activity and various electric phenomenon have from time to time been accused of producing cancer. The increased use of high tension currents is an undoubted fact in modern city life.”
A century later, it is an accepted fact that diabetes and cancer occur together. More than 160 epidemiological studies have investigated this question worldwide, and the majority have confirmed a link between the two diseases. Diabetics are more likely than non-diabetics to develop, and to die from, cancers of the liver, pancreas, kidney, endometrium, colon, rectum, bladder, and breast, as well as non-Hodgkin’s lymphoma.
In December 2009, the American Diabetes Association and American Cancer Society convened a joint conference. The consensus report that resulted concurred: “Cancer and diabetes are diagnosed within the same individual more frequently than would be expected by chance.”
Every historical source shows that cancer always accompanied electricity. In 1914, among about 63,000 American Indians living on reservations, none of which had electricity, there were only two deaths from cancer. The cancer mortality in the United States as a whole was 25 times as high.
An unusual one-year rise in cancer mortality of from 3 to 10 percent occurred in every modernizing country in 1920 or 1921. This corresponded to the beginning of commercial AM radio broadcasting. In 1920, cancer deaths rose 8 percent in Norway, 7 percent in South Africa and France, 5 percent in Sweden, 4 percent in the Netherlands, and 3 percent in the United States. In 1921, cancer deaths rose 10 percent in Portugal, 5 percent in England, Germany, Belgium, and Uruguay, and 4 percent in Australia.
Lung cancer, breast cancer, and prostate cancer rates rose spectacularly throughout the first half of the twentieth century in every country for which we have good data. The number of deaths from breast cancer quintupled in Norway, sextupled in the Netherlands, and increased sixteen-fold in the United States. Lung cancer deaths increase twenty-fold in England. Prostate cancer deaths increased eleven-fold in Switzerland, twelve-fold in Australia, and thirteen-fold in England.
Lung cancer was once so uncommon that it was not even listed separately in most countries until 1929. In the few countries that tracked it, it did not start its dramatic rise until about 1920. Benjamin Ward Richardson, in his 1876 book, Diseases of Modern Life, is surprising to a modern reader in this respect. His chapter on “Cancer from Smoking” discusses the controversy over whether tobacco smoking caused cancer of the lip, tongue, or throat, but cancer of the lung is not even mentioned.
Lung cancer was once so uncommon that it was not even listed separately in most countries until 1929. In the few countries that tracked it, it did not start its dramatic rise until about 1920. Benjamin Ward Richardson, in his 1876 book, Diseases of Modern Life, is surprising to a modern reader in this respect. His chapter on “Cancer from Smoking” discusses the controversy over whether tobacco smoking caused cancer of the lip, tongue, or throat, but cancer of the lung is not even mentioned.
Lung cancer was still rare in 1913, the year when the American Society for the Control of Cancer was founded. Out of 2,641 cases of cancer reported to the New York State Institute for the Study of Malignant Disease that year, there was only a single case of primary lung cancer. Frederick Hoffman, in his exhaustive 1915 book, The Mortality From Cancer Throughout the World, asserted as a proven fact that smoking caused cancer of the lips, mouth, and throat, but like Richardson four decades previously made no mention of lung cancer in connection with smoking.
Swedish researchers Örjan Hallberg and Olle Johansson have shown that the rates of lung, breast, and prostate cancer continued to rise, just as spectacularly, in the second half of the twentieth century in forty countries, along with malignant melanoma and cancers of the bladder and colon—and that the overall rate of cancer changed precisely with changes in the exposure of the population to radio waves.
The rate of increase in cancer deaths in Sweden accelerated in 1920, 1955, and 1969, and took a downturn in 1978. “In 1920 we got AM radio, in 1955 we got FM radio and TV1, in 1969-70 we got TV2 and colour TV and in 1978 several of the old AM broadcasting transmitters were disrupted,” they note in their article, “Cancer Trends During the 20th Century.” Their data suggest that at least as many cases of lung cancer can be attributed to radio waves as to smoking.
The same authors have focused on FM radio exposure in connection with malignant melanoma, following up on the findings of Helen Dolk at the London School of Hygiene and Tropical Medicine. In 1995, Dolk and her colleagues had shown that the incidence of skin melanoma declined with distance from the powerful television and FM radio transmitters at Sutton Coldfield in The West Midlands, England. Noting that the FM frequency range, 85 to 108 MHz, is close to the resonant frequency of the human body, Hallberg and Johansson decided to compare melanoma incidence with exposure to FM radio waves for all 565 Swedish counties. The results are startling.
When melanoma incidence is plotted on a graph against the average number of FM transmitters to which a municipality is exposed, the points fall on a straight line. Counties that get reception from 4 to 5 FM stations have a rate of malignant melanoma that is eleven times as high as counties that do not get reception from any FM station.
Hallberg & Johansson 2005:

In their article, “Malignant Melanoma of the Skin—Not a Sunshine Story,” they refute the notion that the tremendous increase in this disease since 1955 is caused primarily by the sun. No increase in ultraviolet radiation due to ozone depletion occurred as early as 1955. Nor, until the 1960s, did Swedes begin to travel to more southerly countries in large numbers to soak up the sun.
The embarrassing truth is that rates of melanoma on the head and feet hardly rose at all between 1955 and 2008, while rates for sun-protected areas in the middle of the body increased by a factor of twenty. Most moles and melanomas are now occurring not on the head, arms, and feet, but in areas of the body that are not exposed to sunshine.
Elihu Richter, in Israel, has recently published a report on 47 patients, treated at Hebrew University-Hadassah School of Medicine, who developed cancer after occupational exposure to high levels of electromagnetic fields and/or radio waves. Many of these people—especially the youngest people—developed their cancers within a surprisingly short period of time—some as short as five or six months after the beginning of their exposure. This dispelled the notion that we must wait ten or twenty years to see the effects of cell phones on the world’s population. Richter’s team warns that “with the recent introduction of WiFi into schools, personal computers for each pupil in many schools, high frequency voltage transients measured in schools—as well as the population-wide use of cellphones, cordless phones, some exposure to cellphone towers, residential exposure to RF/MW from Smart Meters and other ‘smart’ electronic equipment at the home and possibly also ELF exposures to high power generators and transformers—young people are no longer free from exposure to EMF.”
The range of tumors in Richter’s clinic ran the gamut: leukemias, lymphomas, and cancers of the brain, nasopharynx, rectum, colon, testis, bone, parotid gland, breast, skin, vertebral column, lung, liver, kidney, pituitary gland, pineal gland, prostate, and cheek muscle.
Rate of Rural Cancer in 1931
The graph below shows Cancer deaths (per 100,000 population) based on the percentage of electrification in1931:

Below shows the above totals on the left for 1931 as a list with totals for 1940 on the right:

You may notice that the position of Nevada shifted more than any other state between 1931 and 1940. For some reason, deaths from heart disease, diabetes, and cancer rose dramatically in Nevada while the rate of household electrification rose only modestly. The construction of Hoover Dam, completed in 1936, was that reason. The most powerful hydroelectric plant in the world at that time, its one billion watt capacity supplied Las Vegas, Los Angeles, and most of Southern California via high voltage power lines that coursed through southeastern Nevada on their way to their destinations, exposing the surrounding area—where most of the population of the state lived—to some of the world’s highest levels of electromagnetic fields. In June of 1939 the Los Angeles grid was connected to Hoover Dam via a 287,000-volt transmission line, also the most powerful in the world at that time.
Power lines from Hoover Dam carry electricity to the Los Angeles area:

Two types of cancer deserve additional comment: lung cancer and brain cancer.
The percentage of adults who smoke has declined steadily since 1970 among both men and women. Yet lung cancer mortality has almost quadrupled in women, and is virtually the same in men as it was fifty years ago.
As the following graph shows, the percentage of adults who smoke has declined steadily since 1970 among both men and women. Yet lung cancer mortality has almost quadrupled in women, and is virtually the same in men as it was fifty years ago.

When non-smoker Dana Reeve, the 46-year-old widow of “Superman” actor Christopher Reeve, died of lung cancer in 2006, the public was stunned because we had had it drummed into us for decades that this type of cancer is caused by smoking. Yet lung cancer in people who have never smoked—if you consider it as a separate category—ranks today as the seventh most common cause of cancer deaths worldwide, even before cancer of the cervix, pancreas, and prostate.
Brain tumors deserve mention because, obviously, of cell phones. Several billion people in the world are exposing their brains for up to hours per day to microwave radiation at point blank range—a new situation that began in approximately 1996 or 1997 in most countries. Yet honest data on brain tumors are difficult to obtain because special interests have controlled most of the research funding on brain tumors since the advent of digital cell phones two decades ago. As a result, a media war has pitted the independent scientists, who report a tripling to quintupling of brain cancer rates among those who have used their cell phones for ten years or more, against industry scientists who report no increase in cancer at all.
The problem, as Australian neurosurgeon Charlie Teo tells those who will listen, is that all the data on cell phone usage comes from databanks controlled by cell phone providers, and “no telcos have allowed scientists access to their records for these large studies.”
In 2006 an industry-funded study was published in Denmark, purporting to show not only that cell phones did not cause brain cancer, but that cell phone users even had a lower rate of brain cancer than everyone else. In other words, those scientists would have the world believe that people might actually protect themselves from brain tumors by holding a cell phone to their heads for hours per day. The study, published in the Journal of the National Cancer Institute, was titled “Cellular Telephone Use and Cancer Risks: Update of a Nationwide Danish Cohort.”(Schüz et al. 2006) It claimed to come to its conclusions after an examination of the medical records of over 420,000 Danish cell phone users and non-users over a period of two decades. Although the study found a lower rate of brain cancer—in men only—among cell phone users than non-users, it found a higher rate of exactly those cancers that Swedish scientists Hallberg and Johansson had reported to be caused by radio waves: bladder cancer, breast cancer, lung cancer, and prostate cancer. The Danish study did not report rates of colon cancer or melanoma, the other two types of cancer that the Swedish researchers had mentioned. However, the Danish study did additionally find that testicular cancer in men was higher and that cervical and kidney cancers in women were significantly higher among the cell phone users. Data in the study was clearly manipulated, because the only type of cancer for which a “protective” effect was reported was the type of cancer these scientists and their funders were trying to convince the public that cell phones did not cause: brain cancer.
All of the study’s subjects had actually been using cell phones for a long time by the year 2004, when the study ended. The only difference between “users” and “non-users” was the date of first subscription: the “users” first bought a cell phone between 1982 and 1995, while the “non-users” didn’t buy one until after 1995. And all the “users” were lumped together.
The study did not distinguish between people who had used cell phones for 9 years and people who had used them for 22 years. But according to the study, those who subscribed prior to 1994 tended to be wealthier, and drank and smoked much less, than those who first subscribed later. Controlling for length of use might change the results of the study.
Meanwhile, Dr. Teo is sounding the alarm. “I see 10 to 20 new patients each week,” he says, “and at least one third of those patients’ tumors are in the area of the brain around the ear. As a neurosurgeon I cannot ignore this fact.”
Many if not most of us have one or more acquaintances or family members who have, or have died from, a brain tumor. All of us have heard about famous people who have died of brain tumors—Senator Ted Kennedy, attorney Johnnie Cochran, journalist Robert Novak, Vice President Joe Biden’s son Beau.
Yet highly publicized studies assure us that brain tumor rates are not increasing. This is certainly not true, and a little investigation shows why the data cannot be trusted, in the United States or anywhere else. In 2007, researchers at the Swedish National Board of Health and Welfare found out that, for some reason, one-third of the cases of brain cancer diagnosed at university hospitals, and the majority of cases at county hospitals, were not being reported to the Swedish Cancer Registry.
All other types of cancer were being routinely reported, but not brain cancer.
A 1994 study revealed that difficulties in brain cancer reporting were already occurring in Finland. Although the Finnish cancer registry was complete for most types of cancer, it seriously under reported brain tumors.
Here in the United States, severe problems have been found with surveillance not just of brain cancer, but across the board. The Surveillance Epidemiology and End Results (SEER) program, run by the National Cancer Institute, depends on state registries to deliver accurate data. But the data are not accurate. American researcher David Harris reported at a conference in Berlin in 2008 that state registries cannot keep up with the increasing load of cancer cases because they are not receiving enough funding to do so. “SEER registries are currently faced with the challenge of collecting more cases in less time with often the same limited resources as the previous year,” he said. This means that the greater the rise in cancer, the less it will be reported, barring an improvement in the American economy.
Even worse has been the deliberate refusal by Veterans Administration hospitals and military base medical facilities to report cases to the state cancer registries. A report by Bryant Furlow that appeared in The Lancet Oncology in 2007 noted “a precipitous decline in VA reporting of new cases to California cancer registries beginning in late 2004—from 3,000 cases in 2003 to almost none by the end of 2005.” After inquiring in other states, Furlow discovered that California was not an exception. The Florida cancer registry had never received any VA case reports, and VA facilities in other states were dealing with years of backlogged, unreported cancer cases. “We’ve been working with the VA for more than 5 years, but it’s just got worse,” Holly Howe told him. She represents the North American Association of Central Cancer Registries. As many as 70,000 cases of cancer from the VA were not being reported each year. And in 2007, the VA made non-reporting official policy when it issued a directive on cancer nullifying all existing agreements between state registries and VA facilities. Furlow reported that the Department of Defense was also not cooperating with the cancer registries.
No cancers diagnosed at military base facilities had been reported to any state registries for several years. As a result of all these failures, Dennis Deapon of the Los Angeles Cancer Surveillance Program warned that studies based on the deficient data may be worthless.
“Research from the mid-2000’s will forever require an asterisk, or perhaps a sticker on the cover, to remind researchers and the public that they are not correct,” he said.
Doctors at the Southern Alberta Cancer Research Institute at the University of Calgary were shocked when records showed a 30 percent increase in malignant brain tumors in Calgary in the single year between 2012 and 2013, despite official government statistics proclaiming no rise in malignant brain tumor rates at all in either the province of Alberta or the nation of Canada. This discrepancy has lit a fire under Faith Davis, professor of epidemiology at the University of Alberta’s School of Public Health. As unreliable as official statistics are for malignant tumors, they are even worse for non-malignant tumors: Canada’s surveillance system does not record them at all. To remedy this incredible situation, the Brain Tumour Foundation of Canada announced in July 2015 that it is raising money to help Davis create a national brain tumour registry that will finally give clinicians and researchers access to accurate information.
The studies that are assuring us that all is well with cell phones have been funded by the telecommunications industry. But, and in spite of severe under reporting of brain tumors, independent scientists are confirming the impression of brain surgeons and oncologists that their caseloads are increasing, as well as the evident fact that many more people that we all know and hear about are dying of such tumors than ever before. The most prominent of these independent scientists is Lennart Hardell.
Hardell is a professor of oncology and cancer epidemiology at University Hospital in Örebro, Sweden. Although most of his earlier research was on chemicals like dioxins, PCBs, flame retardants, and herbicides, since 1999 he has focused on exposure to cell and cordless telephones.
He tells us, based on case control studies involving over 1,250 people with malignant brain tumors, that using both cell phones and cordless phones significantly increases one’s risk for brain cancer.
The more years you use such a phone, the more cumulative hours you use one, and the younger you are at first exposure, the greater the odds that you will develop a tumor. Two thousand hours of cell phone use, according to Hardell, triples one’s risk. Two thousand hours on a cordless phone more than doubles one’s risk. First use of a cell phone before the age of twenty increases one’s overall risk of brain cancer three-fold, the risk of an astrocytoma—the most common type of malignant brain tumor—five-fold, and the risk of an astrocytoma on the same side of the head as the phone eight-fold. First use of a cordless phone before the age of twenty doubles the risk of any brain tumor, quadruples the risk of an astrocytoma, and increases the risk of an astrocytoma on the same side of the head eight-fold.
The literature on cell towers and radio towers is less compromised. Almost all of the existing studies, until recently, have been funded by independent sources and not by the telecommunications industry, and they have yielded consistent results: living near a transmission tower is carcinogenic.
William Morton, at Oregon Health Sciences University, found that living near VHF-TV broadcast antennas was a significant risk for leukemia and breast cancer in the Portland-Vancouver metropolitan area from 1967 to 1982.
In 1986, the Department of Health of the State of Hawaii found that residents of Honolulu who lived in census tracts that had one or more broadcast towers had a 43 percent increased risk for all types of cancer.
In 1996, Bruce Hocking, an occupational physician in Melbourne, analyzed the childhood cancer incidence for nine Australian municipalities in relation to a group of three high-power television towers. Children who lived closer than four kilometers to the towers were almost two and a half times more likely to die of leukemia as children in more distant cities.
In 1997, Helen Dolk and her colleagues found high rates of adult leukemia, bladder cancer, and skin melanoma near the Sutton Coldfield tower at the northern edge of Birmingham. When Dolk expanded her study to include twenty high power transmission towers throughout Great Britain, she found that, in general, the closer you lived to a tower, the more likely you were to have leukemia.
In 2000, Neil Cherry analyzed the childhood cancer rate in San Francisco as a function of distance from Sutro Tower. Sutro Tower is almost 1,000 feet tall, stands on top of a tall hill, and can be seen from all over San Francisco. At the time of Cherry’s study it was broadcasting nearly one million watts of VHF-TV and FM radio signals, plus over 18 million watts of UHF-TV. The rates of brain cancer, lymphoma, leukemia, and all cancers combined, throughout San Francisco, were related to the distance a child lived from that tower. Children who lived on hills and ridgetops had much more cancer than children who lived in valleys and were shielded from the tower. Children who lived less than one kilometer from the tower had 9 times the rate of leukemia, 15 times the rate of lymphoma, 31 times the rate of brain cancer, and 18 times the total cancer rate, as children in the rest of the city.
Horst Eger, a physician in Naila, Germany examined 1,000 patient records in his home town. He found that people who lived within 400 meters (1,300 feet) of a cell tower had triple the risk of developing cancer, and developed their cancer, on average, when they were eight years younger, compared to people who lived further away.
In 2011, Adilza Dode headed up a team of university scientists and government officials of a metropolis in southeastern Brazil that confirmed the results of all the previous studies. The risk of cancer for the residents of Belo Horizonte decreased uniformly and steadily with distance from a cell tower.
And on February 24, 2011, the Supreme Court of Italy upheld the 2005 conviction of Cardinal Tucci for polluting Rome with radio waves. A ten-day suspended jail sentence was his only punishment. No one has ever been compensated for their injuries. The Prosecutor’s Office has not filed charges of negligent homicide. Vatican Radio’s antennas have not been shut down.
As a final note, the supposed Covid-19 ‘vaccines’ contain graphene oxide which severely damages the red blood cells, decreasing the amount of oxygen that is carried by the blood, creating varying degrees of hypoxia in those who took the shots. And turbo cancers have become common as one of the results.
For more information on graphene and its damaging effects, use the link below:
Graphene Is The 'Vaccine' Killer
Fabulous riveting transparant ..timely commentary.**
Turbocancers explode..emf radiation..microelectric radiation..graphene oxides mercury iron aluminum..msg..GMO s..glyphosate. 5G.. to 10G.....add unrequested aerosol stratospheric injections....not oil..but benzine...**chromium dioxide.....!,We stumbled across this stellar article....our little complimentary point is ....the religion of white coated lyshenkoist
science whores are not concerned with cancer or any quality of life( for biological humans). type issues..they are in a blinding rush to solve problems that don't texist ..like the fabled ...supposed use of quantum computer nonsense..**...to get medical -..military industrial misdirection-complex...money...white coated anti spiritual--"experts in deed!. Frankinsteen pseudo science in service to ultimate cyborgic NJO totalitarianism. via money laundering and expropriated taxes....is their actual goal.
Outstanding!
Although Warberg was incorrect, oxygen deficiency does not cause cancer.
Oxygen - is dry air - see Jane 333' s research, which is brilliant.
Acute radiation is a dehydrator, the EMF's breaking the structure of water (crystalline in nature) therefore "becoming" oxygen....
It's the dissolving of salt in the atmosphere that causes dehydration of the cell.
The fire triangle.
Less oxygen requires more fuel or heat (glucose being the fuel, heat being body temp for cell replication.
Acute radiation sickness is the tumor causing agent that "dehydrates" the cell causing the body to compensate by additional glucose delivery, the result of a failed replication leaves the acid soup sack we call a tumor.
That's Cancer solved then.
EMF' s and dehydration (low salt levels) cause malfunctioning cell replication aka Cancer
Why they had "salt baths" back int day, and little emfs, thus no cancer.
Cheers guys, that's one for the Good Book 👍
P.s. I would imagine diabetics have a low salt or suger level, exposed to emfs.
P.p.s I also think nitrogen and argon would be in the mix 😂
A very big cheers 🥂
Kind regards,
Michael.